Build a bridge to heal the healthcare workforce
- The crisis of trust that existed between frontline nurses and leadership before the pandemic continues to worsen with evidence of physical, emotional, and moral suffering.
- Trust is innately abstract, but the Reina Three Dimensions of Trust—Trust of Character, Communication, and Capability —can serve as a behavioral-based blueprint that makes trust tangible, practical, and actionable.
The crisis of trust that existed in healthcare before the COVID-19 pandemic has become inescapable. Throughout the pandemic and before, we’ve experienced myriad examples of the costs of working in circumstances that call clinicians to go beyond what’s physically, emotionally, spiritually, and morally justified or healthy. The evidence of physical depletion, burnout, moral suffering, compassion fatigue, degraded mental health, and suicide among clinicians is sobering.
We see examples of the deepening divide between leaders and frontline workers in narratives that reflect resentment, anger, despair, disengagement, grief, and quitting. Data documenting a pervasive erosion of trust and the resulting intensity of moral injury symptoms can’t be ignored. The pattern of these dynamics invites us to ask why trust matters, how it’s broken, and how can it be rebuilt.
Battle of COVID-19: Frontline nurses feel abandoned during the pandemic
8 lessons learned from the COVID-19 pandemic
Why trust matters
Trust is reciprocal and built step-by-step over time. Because it fuels a core human need to connect—to trust and be trusted—it stirs emotions in everyone. Trust is innately abstract, but people feel the power of its presence and the pain of its absence.
When trust is present, energy is expansive. By trusting one another, clinicians continue to do the seemingly impossible—with heart, soul, and commitment. When that foundation of trust becomes vulnerable, people gradually lose confidence in the quality of care provided, doubt decisions, and ask, “How long can I continue?” and “Is this the place for me?” At the threshold of pain and confusion that comes with the erosion of trust, we ask the deepest question, “Is this my reason for being?” “Why did I become a nurse or physician?” These questions coincide with the existential questions that accompany moral injury, a corrosive form of moral suffering.
Trust meets a core human need for connection. People need to be seen, heard, and understood for who they are, what they represent, and for what they bring to their work and their life’s calling. As the source for human connection, trust requires awareness, constant attention, and sound intent. Because trust can be broken so easily, we should never take it for granted.
Understanding the vulnerability of trust requires us to first understand how trust is cultivated. We use the word “trust” easily and speak about it frequently. Some fall prey to the assumption that our role, title, or expertise earns us the trust of others. In relationships, however, only one thing builds trust—how we show up and behave.
The research-based construct of the Reina Three Dimensions of Trust® (the 3Cs)—Trust of Character, Communication, and Capability—provides a behavioral-based blueprint that makes trust tangible, practical, and actionable. All three are grounded in one’s capacity for trust. The model has been applied in over 300 organizations, including financial services, technology, entertainment, transportation, federal government, and in healthcare. Normative data from psychometrically developed assessments that measure trust at the leadership, team, and organizational levels have demonstrated that focusing on targeted behaviors in these three areas is instrumental in building trust and rebuilding it when it’s broken. (See The 3Cs.)
The 3Cs
The Reina Three Dimensions of TrustSM serve as a framework for enhancing organizational trust.
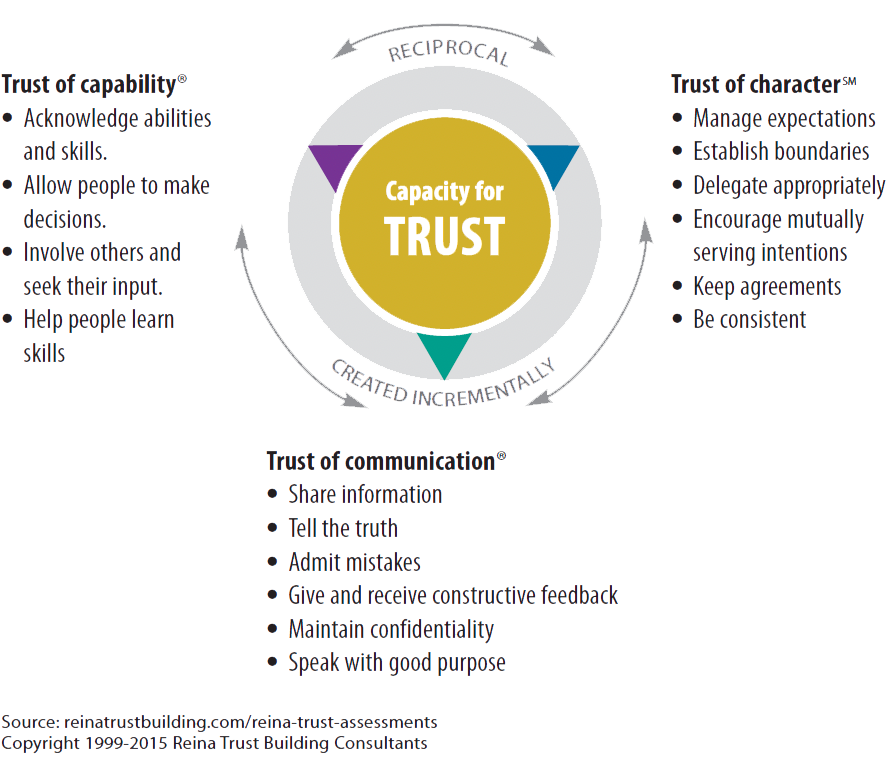
Trust of character
Trust of character sets a tone and direction; it honors the needs of people to be and do their best. Consistently practicing the behaviors that build trust of character, enables people to know what’s expected of them and what they can expect in return. They understand their roles and responsibilities, keep or renegotiate agreements, and support delegation with required resources. Consistently practicing the behaviors that foster trust of character provides stability, alignment, and care for the human experience during times of change and uncertainty. Without this consistent practice, doubt, confusion, and struggle take over.
Trust of communication
Trust of communication establishes transparency and safety for people to surface issues and concerns with the confidence that they’ll be heard by those who can make a difference. In this atmosphere, people openly express their vulnerabilities and admit their mistakes with a curiosity for the lessons they can learn. Everyone has the information they need to carry out their responsibilities. Development and growth are nurtured through constructive feedback with positive intent rather than as a weapon that ignites fear and shame.
Trust of capability
Trust of capability allows people to leverage their own and one another’s skills, knowledge, experience, and abilities. People involve each other and seek their input, particularly for decisions that affect their jobs and their lives. They take responsibility and support one another to help them learn skills needed to do their jobs and foster their adaptability of skills during extenuating circumstances of uncertainty.
Application of the 3Cs outside of healthcare has demonstrated that the power of human connection made possible through trust drives business performance and manages change. When practiced together, the interrelated 3Cs support the reciprocity of trust that carries the continuity of human connection through change and uncertainty.
Validated tools to measure these dimensions of trust in the context of individuals, teams, organizations, and leadership offer concrete directions for amplifying existing trust-building behaviors and focus attention on those that break trust. Leaders (n=1,248) who engaged in the Reina Leadership Trust Scale® 360-degree assessment identified where they struggle to practice trust-building behaviors. Feedback from 3,974 of their direct reports identified behaviors they experience their leaders struggling to demonstrate. Responses revealed several areas of congruence between leaders and their direct reports. (See Leader vs. direct report appraisals.)
Leader vs. direct report appraisals
When leaders (n=1,248) and direct reports (n=3,974) participated in the Reina Leadership Trust Scale® 360-degree assessment, several
areas of congruence came to light. Bold text reflects behavioral areas of struggle experienced by both leaders and their direct reports in descending order.
Trust-building behaviors that leaders report struggling to practice
- Receiving constructive feedback without getting defensive
- Giving constructive feedback to employees in ways that are timely and helpful
- Setting expectations that are appropriate and perceived as neither too high nor too low
- Providing coaching and feedback on performance when needed
- Giving people the benefit of the doubt
- Giving employees the training necessary to do their jobs
- Challenging employees in ways that motivate them to learn and grow
Trust-building behaviors that direct reports observe leaders struggling to practice
- Giving the benefit of the doubt
- Providing coaching and feedback on performance when needed
- Helping employees learn new skills
- Challenging employees in ways that motivate them to learn and grow
- Taking an active role in employees’ advancement
- Giving employees the training necessary to do their jobs
- Giving constructive feedback to employees in ways that are timely and helpful
Trust serves as the bridge between the business need for performance and the human need for connection. It creates the conditions for mutually serving intentions, ensuring transparent communication, and leveraging the knowledge and skills of the workforce. Although the 3Cs have been applied to healthcare in limited ways, data indicate that we can measure how trust is built and broken in critical care settings. Researchers have used the model to diagnose where trust was being built and broken in a pediatric intensive care unit; consistent with normative data using the scale, communication trust in that unit was consistently the most vulnerable. The model also has been applied to patients and their families, to clinical teams, and as an organizing framework for data analysis and balancing patient experience with staff safety.
How trust breaks
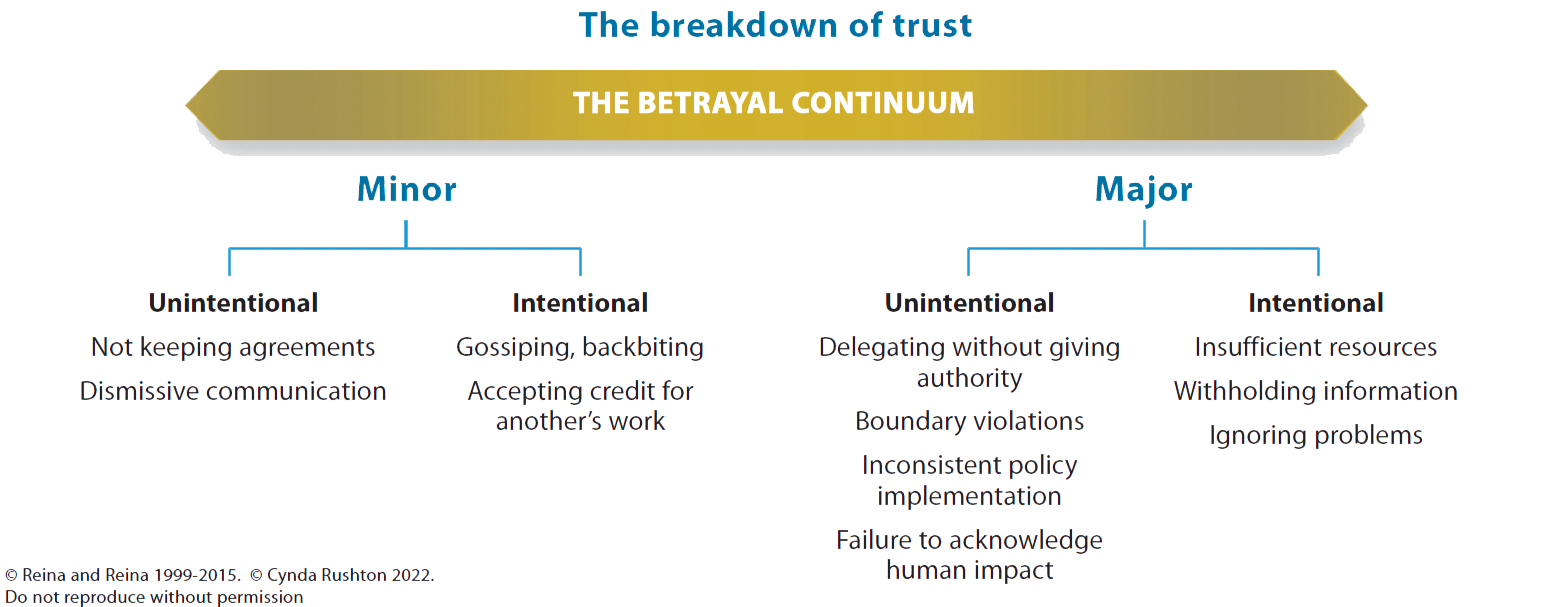
As human beings, we’re imperfect, which makes trust inherently vulnerable. Inconsistently practicing the 3Cs erodes trust. Left unaddressed, people may feel betrayed. Betrayal, a breach of trust or the perception of a breach, occurs along a continuum from minor unintentional acts to major intentional acts. Major breaches cause trust to break down. However, according to Reina and Reina, in relationships, 90% of the events that erode trust are minor breaches that accumulate and become major. When seemingly innocent acts occur repeatedly, they erode trust by a thousand tiny cuts. Their accumulation takes the form of betrayal, which results in anger, resentment, and disengagement. (See Betrayal continuum.)
Betrayal continuum
Trust can break down over time as minor breaches accumulate. Rather than serve as a diagnostic tool, the betrayal continuum provides a reference point for understanding how betrayal emerges through patterns of minor and major breaches of trust.
The following story provides an example of broken trust during the pandemic and demonstrates how behaviors associated with the 3Cs can breech trust.
One nurse’s experience
“I’m not sure what it means to be a nurse anymore,” muses Reese, who’s been working in critical care for the past 4 years—with only a year of experience at the beginning of the COVID-19 pandemic. Today, the second in a 3-day, 12-hour shift assignment, despite not feeling well, Reese decided to come in anyway because of short staffing. Accompanying Reese are two physicians who’ve been working long hours because of a surge of patients in the emergency department (ED), add-on surgery cases, and staff illnesses. The number of patients with COVID has eased slightly, but only after months of daily efforts to care for those who needed critical care. Now everyone is exhausted—some people are angry, others are going through the motions, and others are quitting.
At a town hall meeting, the hospital president expresses relief, saying, “We’re now in the recovery phase of the pandemic.” Mikaela, an ED physician, responds, “We may think we’re in the recovery phase, but it didn’t come without a significant toll on all of us, and we haven’t recovered.” The president declares, “This is just what we do! We always rise to every occasion and make things work!”
This doesn’t ring true to Reese. She thinks, “How could we be in the recovery phase without enough support staff to draw blood, deliver supplies, or transport patients?” Recent talk of the financial impact of the pandemic on the hospital, despite federal relief, leads Reese to wonder, “No one is talking about the impact on the workforce of ‘doing whatever it takes.’” In addition, Reese recently heard about a possible reorganization, which will mean budget cuts and continuing to do more with less. “No one has asked us about what WE think ought to be cut,” thinks Reese. “Instead, we’re informed of the decisions of others.” A recently released video illustrating all the great people in the organization and describing them as heroes struck a chord with Reese, causing her to ask, “How can we be heroes and be asked to work under these circumstances?”
Reese recognizes symptoms of post-traumatic stress disorder and knows she needs help. Reese raises the issue with her nurse manager, who says, “We can’t afford to have anyone else out on sick leave!” She refers Reese to the employee assistance program and offers an extra day off. After trying to get an appointment with a mental health professional for 2 weeks, Reese tells the nurse manager that she needs to take a leave of absence or she’ll have to quit. Reluctantly, the manager grants the leave. Reese tries again to access mental health services through the hospital but has no luck. Only after a mental health colleague intervenes can Reese get an appointment.
Healthcare professionals at all levels of responsibility can see themselves in this story. Perhaps you can relate to the executive who’s attempting to reassure the staff that the worst is behind them. Or you’re a nurse or physician unable to share the positive attitude of the executive as the strain of doing more with less threatens care quality. Or maybe you see yourself as Reese, who’s so depleted and morally injured that she doubts her capacity to function in the emerging status quo.
Regardless of your role, healthcare workers share common ground—the call to serve a higher purpose; to care for the sick, disabled, or dying; to provide care while avoiding harm; and to deliver fair and equitable care. Our professional oaths ground our commitment to respond to the needs of humanity, frequently at great personal sacrifice. This ethos has been lauded as a hallmark of heroes, but as the pandemic has highlighted, it has limitations and vulnerabilities. Leaders betray trust when they take for granted that clinicians will always step up (no matter what) and when systems depend on continuing heroic effort. In addition, clinicians’ deeply held values and commitments can be corrupted to the point where they intentionally or unintentionally undermine behaviors associated with the 3Cs in relation to their leaders, colleagues, and even their patients.
During the pandemic, the lack of uniform standards of care, the uncertain accuracy of information, and the scarcity of resources necessitated undesirable ethical trade-offs and produced a pattern of inconsistency that resulted in unrelenting stress and fear. Clinicians faced unrealistic expectations when tasked with meeting the volume and acuity of their patients but without the usual resources or guidelines and without the opportunity for negotiation. Leaders also faced strain as they bore the responsibility of maintaining the strategic and operational health of their organization.
The vulnerability of trust
Reese’s story reveals the vulnerability of trust. When people feel invisible or unheard, Trust of Communication breaks down. This undermines the human need of those who deliver care to be seen and understood, particularly during this steady state of struggle. In a well-functioning healthcare system, a reciprocal Trust of Character unifies clinicians, their leaders, their organizations, and the public they serve. Amidst the pandemic, when connection and shared purpose were most essential, they eroded.
Reese and her colleagues experienced repeated violations of trust. In the absence of mutually serving intentions, the unrelenting expectation of self-sacrifice degraded clinicians’ mental, emotional, spiritual, and moral health and well-being, which was made increasingly untenable as it became the norm. Eventually, the toll of doing “whatever it takes” unravels clinicians’ Trust of Capability in themselves and their colleagues. When accumulating moral residue goes unrelieved, moral suffering ensues, trust contracts, and patient care and relationships suffer.
The promise of resources, including mental health services, set an expectation of support that wasn’t delivered. Reese had been told each year during open enrollment that she could access a broad array of resources. When she needed them, they evaporated. This, coupled with a guilt-inducing and unsupportive response by her leader, deepened the breach of Trust of Character and Communication that Reese experienced.
Mikaela lost Trust of Communication when she highlighted the costs of providing care with limited resources and was met with an overly optimistic or dismissive response. Messages of brighter times ahead are experienced as hollow and offensive, rather than supportive and encouraging. Superficial messages, such as “The worst is over” or “We’re in the recovery phase,” overlook the lingering impact of years of doing more with less and contribute to another breach of trust.
The erosion of trust that arises from failing to acknowledge the depth of challenge clinicians faced and continue to confront impacts both the quality of patient care and the quality of clinicians’ lives. Leaders may believe that they’re motivating clinicians by directing them to connect to their purpose, but such statements have the unintended consequences of discounting their sacrifices and exploiting the sanctity of their commitment to their patients. Other leaders may be aware of this effect but still resort to the methods of justification that have worked in the past to achieve their goals without recognizing the cost.
Reese lamented that major organizational decisions were being made without the input of the people expected to implement them. Operational decisions during the pandemic needed to be made quickly and without sufficient or reliable information. Perhaps as an unavoidable consequence, clinicians were left out of decisions that impacted work life and quality of care, were assigned tasks without the authority necessary to fulfill them, and were deployed to unfamiliar wards and duties without sufficient training. Taken together, these conditions inevitably eroded all three spheres of trust.
In a steady state of betrayal, questioning and doubt take over. Feeling their best interests are no longer considered, clinicians begin to question the higher calling that brought them into their profession. Without enough support staff to draw blood, deliver supplies, or transport patients, the costs accumulate, and the concurrent narratives of clinicians and leaders “doing whatever it takes” diverge.
Forced to reconcile actions they appraise as disrespectful, unjust, or harmful, clinicians lose touch with the values they profess and the identity they rely on. They begin to believe that the economic force of numbers that demonstrate profit has corrupted their service. In some instances, moral residue, distress, and injury ensue. Feeling irrelevant, unappreciated, stripped down to their core, and perceiving they have no power, control, or choice, clinicians may choose to leave their role, their job, or their profession. Others may stay, go through the motions, assume a state of detached resignation, or join the ranks of the working wounded.
How to rebuild trust
The breakdowns of trust illustrated in Reese’s story require intentional actions and behaviors to rebuild it. The Seven Steps for Rebuilding Trust®, a foundational framework used in other sectors, helps leaders and others demonstrate courage and take concrete, constructive, and compassionate action. In the healthcare setting, the process can help heal the betrayals experienced during the pandemic. (See Rebuild trust: Step by step.)
1. Observe and acknowledge what’s happened
Healing a breach of trust begins by facing the reality of the violation. In Reese’s case, the pandemic assailed clinicians’ trust in their leaders, their organization, their colleagues, and themselves. To address those betrayals, leaders must expressly recognize the tremendous toll on the workforce. System leaders must acknowledge the broken promise of resources and mental health support they failed to provide. In addition, clinicians must face and name the compromises to the care they provided to their patients and themselves.
2. Allow feelings to surface
People experience the impact of a breach of trust embedded in change as a loss—the loss of what was or what could have been. Loss and betrayal can engender a range of feelings, including anger, resentment, blame, shame, guilt, anxiety, or self-righteous indignation. Clinicians require a forum in which they can express these negative and discomforting emotions. Leaders must bear witness to these reactions without rationalization, excessive explanation, or justification.
3. Get and give support
Support helps us gain perspective and move through the pain of lost trust to trust again. Leaders must create psychologically safe and confidential environments for clinicians to express the emotions that accompany betrayal without fixing or consoling. Focus groups, team meetings, and one-on-one conversations create safe forums to ensure that employees’ emotions don’t go underground. The use of a skilled facilitator may help. Leaders are human beings, too. They know that the decisions they make come with consequences. To support themselves, leaders may want to access a trusted advisor or executive coach to promote their own healing and prepare them to hold the discomforting revelations of their staff.
4. Reframe the experience
Sharing and listening with compassion allow clinicians and leaders the opportunity to take on new perspectives. Clinicians can learn about the larger context of extenuating circumstances and business reasons behind a set of decisions. Leaders can appreciate the intended or unintended consequences of their decisions on the workforce. When supported, people can reframe betrayal as a gift or a teacher. Reframing hardship together defines the challenge and builds a foundation for co-creating the steps to address it together.
5. Take responsibility
Healing to rebuild trust asks that each person own up to their role. Integrity requires that everyone acknowledge how they respond and co-create the path forward. Even when you’re responsible for what happened, practicing the 3Cs can help you take responsibility for your own path forward and empower others to do so as well. Everyone may need to check their assumptions, suspend judgment, and ask questions for perspective and understanding. Taking responsibility may include an authentic apology, identifying lessons learned, taking actions to improve the current situation, and establishing safeguards to avoid similar situations in the future.
6. Forgive yourself and others
Forgiveness is the inner work of healing. Forgiving doesn’t mean excusing; it means acknowledging the impact of broken trust and agreeing not only to move through it but also to learn from it. Forgiveness takes time and can’t be forced. It’s essential to restoring integrity and healing after a betrayal. Each person’s capacity to forgive themselves and others reflects their history of trust built and broken. Through forgiveness, people can release bitterness, resentment, and doubt. Rather than remaining stuck in the past or current struggle, they look ahead.
7. Help people let go and move on
As humans, we tend to hold onto resentments, hurts, and betrayals. Our nervous system continues to detect threats, which makes it more difficult to release negative emotions and move forward. Accepting what’s happened doesn’t mean that we agree with or overlook its significance. Clinicians won’t forget what happened, but they can choose to look forward rather than remain stuck in the past. Letting go and moving on cements the insights, lessons, and perspective gained through healing.
Restore humanity and trust
Trust sits at the center of the human dynamic within healthcare, which makes it innately vulnerable. Change, uncertainty, and ambiguity further punctuate that vulnerability. However, these challenging dynamics don’t have to erode trust permanently. The Three Dimensions of Trust raise awareness of human behavior and provide a common language and shared understanding to help people at all levels of responsibility openly and constructively talk about trust-related dynamics. With the benefit of insight and a behavioral construct that can take action to build trust, the 3Cs offer a promising framework for identifying areas where robust trust behaviors exist and also where trust is broken.
Commitment to practicing the Three Dimensions of Trust with sound intent as well as stepping into and working through the Seven Steps to Rebuild Trust honor the human need to heal and renew the spirit of relationships. These steps also support organizational leadership as it sets a course for trust sustained over time. Together, clinicians and leaders have an opportunity to transform the betrayals exacerbated by the pandemic and co-create practice environments where humanity and trust are restored.
Cynda Hylton Rushton is the Anne and George L. Bunting Professor of Clinical Ethics and Nursing at Johns Hopkins University in Baltimore, Maryland. Michelle Reina is the CEO and co-founder of Reina Trust Building, a global consultancy based in in Stowe, Vermont.
American Nurse Journal. 2024; 19(5). Doi: 10.51256/ANJ052424
References
Dean W, Talbot S, Dean A. Reframing clinician distress: Moral injury not burnout. Fed Pract. 2019;36(9):400-2.
LeClaire M, Poplau S, Linzer M, Brown R, Sinsky C. Compromised integrity, burnout, and intent to leave the job in critical care nurses and physicians. Crit Care Explor. 2022;4(2):e0629. doi:10.1097/CCE.0000000000000629
Mantri S, Song YK, Lawson JM, Berger EJ, Koenig HG. Moral injury and burnout in health care professionals during the COVID-19 pandemic. J Nerv Ment Dis. 2021;209(10), 720-6. doi:10.1097/NMD.0000000000001367
National Academy of Medicine. Taking Action Against Clinician Burnout: A Systems Approach to Professional Well-Being. Washington, DC: National Academies Press; 2019.
Nelson KE, Hansen GC, Boyce D, et al. Organizational impact on healthcare workers’ moral injury during COVID-19: A mixed-methods analysis. J Nurs Adm. 2022;52(1):57-66. doi:10.1097/NNA.0000000000001103
Reina D, Reina M. Trust and Betrayal in the Workplace: Building Effective Relationships in Your Organization. Oakland, CA: Berrett-Koehler; 2015.
Reina DS, Reina ML. Leaders and their Direct Reports Identify Leaders’ Most Problematic Trust Behaviors research report. 2024. https://reinatrustbuilding.com/reina-trust-assessments.
Reina ML, Reina DS, Rushton CH. Trust: The foundation for team collaboration and healthy work environments. AACN Adv Crit Care. 2007;18(2):103-8. doi:10.4037/15597768-2007-2002
Rushton CH. Transforming moral suffering by cultivating moral resilience and ethical practice. Am J Crit Care. 2023;32(4):238-48. doi:10.4037/ajcc2023207
Rushton CH, Nelson KE, Antonsdottir I, Hanson GC, Boyce D. Perceived organizational effectiveness, moral injury, and moral resilience among nurses during the COVID-19 pandemic. Nurs Manage. 2022;53(7):12-22. doi:10.1097/01.NUMA.0000834524.01865.cc
Rushton CH, Reina ML, Francovich C, Naumann P, Reina DS. Application of the Reina Trust and Betrayal Model® to the experience of pediatric critical care clinicians. Am J Crit Care. 2010;19(4):e41-51. doi:10.4037/ajcc2010323
Rushton CH, Reina ML, Reina DS. Building trustworthy relationships with critically ill patients and families. AACN Adv Crit Care. 2007;18(1):19-30. doi:10.4037/15597768-2007-1004
Rushton CH, Thomas TA, Antonsdottir IM, et al. Moral injury and moral resilience in health care workers during COVID-19 pandemic. J Palliat Med. 2022;25(5):712-9. doi:10.1089/jpm.2021.0076
Rushton CH, Turner K, Brock RN, Braxton JM. The invisible moral wounds of the pandemic: Are we experiencing moral injury? AACN Adv Crit Care. 2021;35(1):119-25. doi:10.4037/aacnacc2021686
Rushton CH, Wood LJ, Grimley K, Mansfield J, Jacobs B, Wolf JA. Rebuilding a foundation of trust: A call to action in creating a safe environment for everyone. Pt Exp J. 2021;8(3):5-12. doi:10.35680/2372-0247.1651
Schlak AE, Rosa WE, Rushton CH, Poghosyan L, Root MC, McHugh MD. An expanded institutional- and national-level blueprint to address nurse burnout and moral suffering amid the evolving pandemic. Nurs Manage. 2022;53(1)16-27. doi:10.1097/01.NUMA.0000816956.46367.71
Spilg EG, Rushton CH, Phillips JL, et al. The new frontline: Exploring the links between moral distress, moral resilience and mental health in healthcare workers during the COVID-19 pandemic. BMC Psychiatry. 2022;22(1):19. doi:10.1186/s12888-021-03637-w
Swavely D, Romig B, Weissinger G, et al. The impact of traumatic stress, resilience, and threats to core values on nurses during a pandemic. J Nurs Adm. 2022;52(10):525-35. doi:10.1097/NNA.0000000000001194
U.S. Department of Health and Human Services. Addressing Health Worker Burnout: The U.S. Surgeon General’s Advisory on Building a Thriving Health Workforce. 2022. hhs.gov/sites/default/files/health-worker-wellbeing-advisory.pdf
Key words: trust, broken trust, COVID-19, pandemic, frontline nurses, moral injury, compassion fatigue