The KIND study reviews nurses’ knowledge and understanding of intravascular volume.
- A knowledge deficit exists among nurses regarding the understanding of hemodynamic and intravascular fluid status and monitoring.
- The Knowledge of INtravascular Determination (KIND) study aimed to understand the knowledge of frontline RNs regarding fluid status and fluid responsiveness and the use of associated technologies.
- Nurses in all clinical areas still rely heavily on traditional, inaccurate monitoring.
A knowledge deficit exists among nurses and other clinicians regarding intravascular fluid status monitoring. Several studies indicate that clinicians don’t adequately understand the principles of fluid status assessment. Connors and colleagues identified that clinician lack of understanding and variation in monitoring methods lead to inconsistent clinical assessment and fluid therapy management practices. (See Volume status vs. fluid responsiveness.)
Volume status vs. fluid responsiveness
A difference exists between a patient’s volume status and their body’s ability to respond to fluid therapy (fluid responsiveness). Volume status refers to the volume of blood circulating in the intravascular system. Fluid responsiveness indicates an increase in stroke volume of 10%
to 15% after administering a fluid bolus or physiologic bolus with a passive leg raise. Clinicians frequently confuse the two, which contributes to inappropriate clinical management.
Current nursing practice uses heart rate (HR), blood pressure (BP), and urine output to monitor intravascular volume and fluid responsiveness. However, stroke volume measurement is the primary hemodynamic response to blood volume changes; HR, BP, and urine output are secondary. Nurses use these secondary responses because they’re easily accessible and convenient. Studies indicate that these secondary responses fail to detect intravascular volume depletion, volume overload, or fluid responsiveness.
Caring for patients receiving vasopressors and inotropes in the ICU
Complete blood count: Getting beyond the basics
The five P’s spell positive outcomes for ARDS patients
Previous research
To improve patient outcomes in response to I.V. fluid, several studies have explored the clinical knowledge and effectiveness of volume status and responsiveness monitoring practices. Connors and colleagues examined the impact of right heart catheterization (pulmonary artery catheters [PAC]) during the first 24 hours in the intensive care unit. They looked at survival, length of stay, intensity, and cost of care. Their findings demonstrated that patients with PACs had an increased 30-day mortality and length of stay plus higher costs. After publication of the study, PACs use declined significantly.
However, clinicians still use static measurements of central venous pressure and pulmonary artery wedge pressure to assess volume status. These parameters aren’t sensitive or specific predictors of the ability of a patient to respond to a fluid bolus, which providers prescribe to correct hypovolemia, hypotension, or inadequate blood flow and ensure adequate tissue perfusion.
According to studies examining nurses’ knowledge and use of PAC, only 50% to 70% correctly understood the technology. Scores varied by clinician training, frequency of use, and the type of medical facility. To prevent end-organ damage, nurses must recognize threats to volume status early.
Measurement technologies
Several technologies (invasive and noninvasive) exist to measure fluid. Minimally invasive measures include pulse pressure variation and stroke volume variation using transesophageal Doppler or an arterial line. Noninvasive, easy-to-use methods to assess stroke volume and fluid responsiveness include bioreactance technology and passive leg raise (PLR). To perform PLR, place the patient in a supine position and elevate both limbs to 45 degrees. Venous blood from the legs and the abdominal compartment increases venous return. A 10% or greater increase in stroke volume in response to PLR predicts fluid responsiveness.
Despite the availability of these technologies, clinical practice remains variable across all areas of practice. Most clinicians administer varied amounts of I.V. bolus fluids in response to a clinical presentation of acute hypotension, regardless of the cause. Studies indicate that approximately 50% of fluid boluses fail to improve cardiac output in unstable patients, and many clinicians struggle to assess individualized fluid management. Determining current clinician knowledge of volume status and fluid responsiveness can help clarify educational needs and reduce clinical practice variation. (See Available technologies.)
Available technologies
Clinicians can use the following noninvasive and invasive technologies to accurately measure cardiac output and stroke volume.
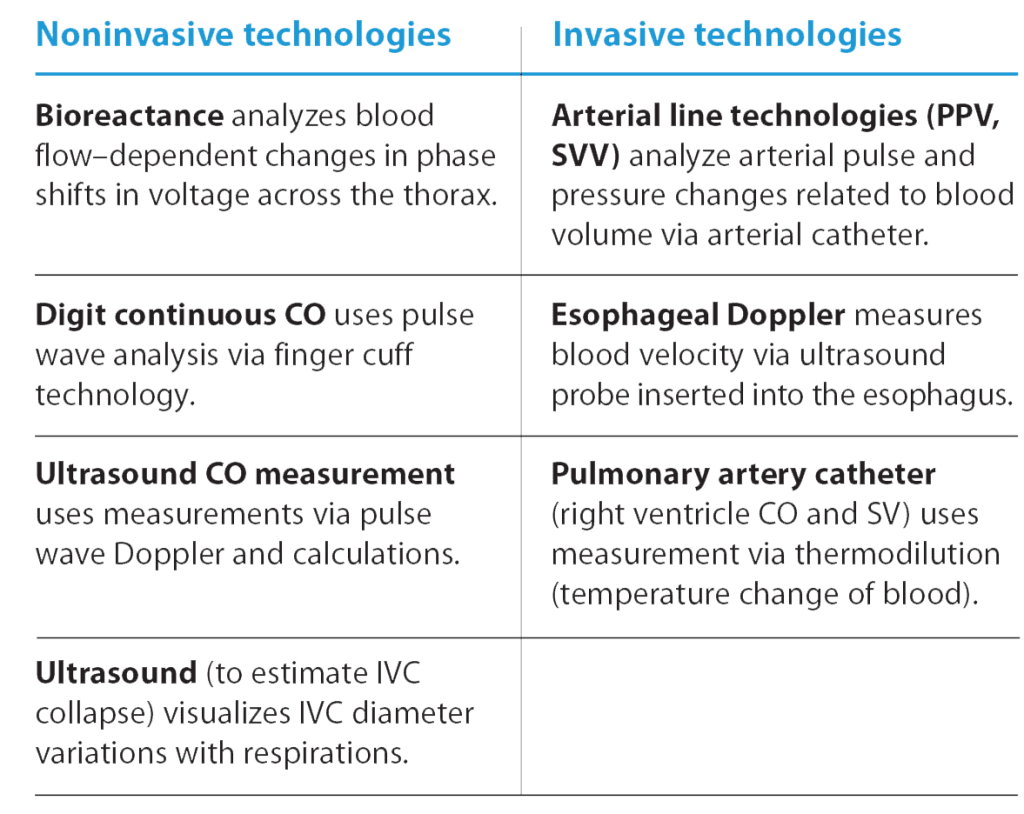
CO = cardiac output, IVC = inferior vena cava, PPV = pulse pressure variation, SV = stroke volume, SVV stroke volume variation
Used with permission of N Kupchik Consulting 2022.
Our goals
We aimed to understand nurse knowledge of volume status, fluid responsiveness, and associated technologies in various clinical areas. We wanted to identify nurses’ knowledge base and ability to differentiate between volume status and fluid responsiveness, evaluate whether they perceive volume status and fluid responsiveness as contradictory or complementary, and determine what measurement strategies and tools they’re currently using. In addition, we wanted to identify any problems or barriers associated with these methods. Six nationally known acute and critical care nurses validated the survey question content.
What we did
We conducted a convenience sample survey of critical care, medical surgical, perioperative, progressive care, and emergency department (ED) nurses via professional organization online communities and email. We didn’t randomize the sample. Eligible participants included members of the Academy of Medical-Surgical Nurses, American Association of Critical-Care Nurses, American Association of Nurse Practitioners, Emergency Nurse Association, American Association of Nurse Anesthesiology, and the National Association of Clinical Nurse Specialists.
We made the survey available to approximately 17,000 nurses. After the initial contact, we sent two reminders over a period of 4 weeks. For informed consent, a short page inviting the nurse to participate preceded the voluntary survey. Survey completion served as consent to participate. (See Survey questions.)
Survey questions
Survey participants answered the following questions (multiple choice, true/false, check all, rank order) related to intravascular volume:
- Mrs. Jones is admitted to your unit. You’re conducting your admission assessment and you’ve been presented with the following information: ins and outs (IOs), weight, chest x-rays, pitting edema, and the presence/absence of crackles in the lungs. What does that information help you assess?
- A normal person is typically fluid responsive.
- A patient is fluid responsive if ________________
- The intravascular volume status of a patient is ___________
- If a patient is fluid response, they must have a low intravascular volume status (hypovolemic).
- If a patient is NOT fluid responsive, they must have a high intravascular volume status (hypervolemic).
- A patient presents with a BP of 84/60 mmHg, HR of 110 beats per minute, respiration rate of 28 breaths per minute, and a temperature of 101.6° F. Without additional definitive data, what approach would you typically take first? ______________________________________
- To assess if a patient is fluid responsive, one would look for an increase of 10% or greater in ____________________ after giving a fluid challenge.
- When assessing intravascular volume status in a hemodynamically unstable patient, which of the following parameters do you routinely use? (Check all that apply.)
- After giving a fluid challenge, how frequently do you use the following parameters to assess if the patient is fluid responsive? (For each parameter or measure, select the best option.)
- Please rank the following parameters in order of usefulness for guiding intravascular fluid management therapy decisions (administering fluids and/or vasoactive drugs) in hemodynamically unstable patients. (For the most useful parameter, select 1, for the next most useful, select 2, etc. Rank five.)
- How frequently do you use the following hemodynamic monitoring technologies to help guide fluid management in your patients? (critical care and ED nurse question)
- On a scale of 1 to 5, rank how strongly you agree with the following statements:
- Having a more accurate measure to help assess volume status is extremely important to me.
- Knowing both a patient’s volume status and if they’re fluid responsive is critical to the care of the patient.
- In my current work environment, a patient’s volume status can be difficult to accurately assess.
- Fluid management (achieving or maintaining hemodynamic stability) is a key component of my job.
See Survey results for the parameters and monitoring technologies
How we analyzed the data
We conducted our analysis using an IBM statistical software suite and used descriptive statistics to describe survey participant characteristics (role as an RN, area of practice, and years in nursing) and to summarize survey responses. We analyzed knowledge questions separately using the frequency and proportion of participants who answered each question correctly. Chi-square tests helped us determine if categorical survey responses differed across area of practice and role as an RN. We used analysis of variance to test differences in responses regarding whether a patient’s volume status is difficult to assess across the nurse’s area of practice. In addition, we conducted multiple comparisons with Bonferroni correction to further explore which areas of practice were different. Statistical significance was set at alpha = 0.05.
What we learned
Out of 15,000 surveys, 916 nurses participated. Of those, 291 completed the full survey. Individuals completing the survey included staff nurses (64.2%), advanced practice nurses (17.9%), and educators, nurse leaders, managers, and directors (17.9%). Practice settings included medical-surgical/stepdown/progressive units (45.9%), critical care (42.8%), perioperative (7.9%), and EDs (3.4%).
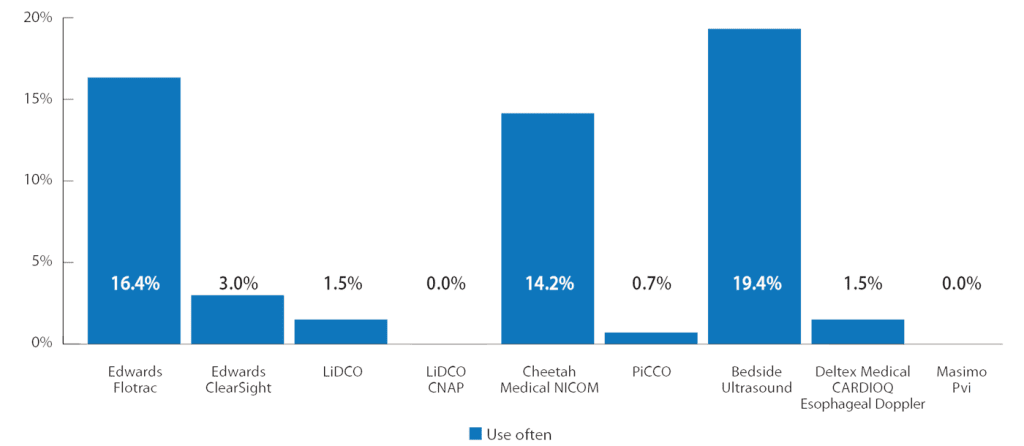
Survey data
Data collected from the survey conducted with nurses regarding intravascular volume indicated the use of secondary parameters (urinary output, heart rate, and mean arterial pressure) rather than the more accurate primary parameters. In addition, results show that most critical care and emergency department nurse respondents don’t use available technology.
Assessment parameters most frequently used by nurses to assess volume status of hemodynamically unstable patients
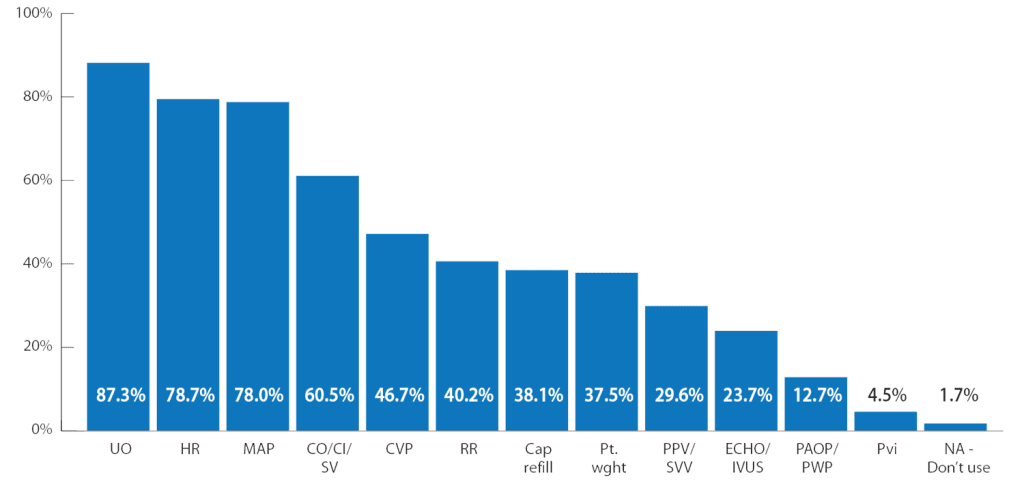
CO/CI/SV = cardiac output/cardiac index/stroke volume, ECHO/IVUS = echocardiogram/intravascular ultrasound, HR = heart rate, MAP = mean arterial pressure, PAOP/PWP = pulmonary artery occlusion pressure/pulmonary wedge pressure, PPV/SVV = pulse pressure variation/stroke volume variation, PVi = pleth variability index, RR = respiratory rate, UO = urine output
ED and critical care nurses reported use of technology
Knowledge
Survey questions 1 through 6 assessed knowledge of volume status and fluid responsiveness (with the first four assessing understanding). Almost all nurses answered these questions correctly, and we noted no statistical differences among clinical areas or roles. Questions 5 and 6 had a significantly low percentage of correct answers in all nurse roles and clinical areas. We determined that the wording of these questions may have been confusing.
We designed question 7 to determine a nurse’s first action when a patient presents with clinical signs of deterioration associated with sepsis. Overall, nurses in all clinical areas and roles answered this question well. We noted no statistical difference among clinical areas or roles.
Assessment strategies and use of clinical parameters
Question 8 examined how nurses would assess fluid responsiveness. This question had a correct response rate below 50% in all clinical areas and roles.
In response to question 9, nurses chose traditional parameters of HR (78.7%), urine output (87.3%), and mean arterial pressure (78%) to assess volume status in a hemodynamically unstable patient. Similarly, in question 10, nurses selected HR (96.2%), urine output (95.2%), and mean arterial pressure (91.8%) to assess fluid responsiveness. In question 11, the parameters listed as most useful for guiding fluid management therapy decisions were the same as those used to assess volume status and responsiveness: HR (73.6%), urine output (73.9%) and mean arterial pressure (72.5%).
Technology use
In question 12, we sought to determine how frequently critical care and ED nurses use hemodynamic monitoring technology to guide fluid management and responsiveness. The results suggest overall low use of any technology, with the most common being pulse contour at 16% and bioreactance at 14.2%. (See Survey data.)
Nurse perception of assessment needs
Question 13 asked nurses to rank how strongly they agree with statements regarding their role in fluid management. All categories of nurses responded favorably, choosing agree or strongly agree to each statement: 89.7% perceive that having a more accurate measure to assess volume is extremely important, 96.2% perceive it’s critical to patient care to know both a patient’s volume status and fluid responsiveness, 63.9% perceive patient volume status as difficult to accurately assess in their current work environment, and 86.3% perceive fluid management as a key component of their job.
What the results tell us
Nurses from 44 states responded to our survey, making it one of the most widespread samplings of nurses ever conducted regarding fluid management. In addition, the inclusion of nurses in all clinical areas helped us gain a better understanding of volume status and fluid responsiveness knowledge. We noted a few key points based on the results.
The data indicate that nurses understand the concept of volume status and fluid responsiveness, but they don’t necessarily understand how to measure them. Nurses in all clinical areas still rely heavily on traditional monitoring of BP, HR, and urine output to evaluate both fluid volume and responsiveness. We found the results disappointing given the number of studies that indicate positive outcomes when using parameters such as stroke volume. Research has repeatedly demonstrated traditional parameters to be less helpful, but they appear to remain the dominant form of assessment.
Nurses would like help to more accurately assess volume status and fluid responsiveness. However, use of hemodynamic technologies in critical care isn’t common. Only about 30% of nurses use technology to guide fluid management. The results indicate lack of noninvasive or minimally invasive monitoring. Nurses can use some types of fluid monitoring, such as bioreactance, in any clinical setting, but study results indicate that they’re not using these technologies.
These results coincide with a recent Canadian study by Crowe, which found that most nurse participants agreed about the importance of I.V. fluids (including type, amount, and rationale for infusion), but that they struggled to recognize how to determine a patient’s volume status vs. fluid responsiveness.
Most undergraduate curriculum and hospital-based acute and critical care courses don’t include education regarding volume status vs. fluid responsiveness. For example, the American Association of Colleges of Nursing (AACN) Essentials of Critical Care Orientation (ECCO), a widely used curriculum, addresses dynamic parameter assessment, but doesn’t clearly define the difference between volume status and fluid responsiveness. To our knowledge, no clear standards exist regarding fluid administration in nursing schools or hospitals. In addition, concepts such as vascular permeability, contractility, and elasticity may not be taught well, if at all.
Several factors may contribute to nurses’ difficulty assessing the need for fluid. For example, when deciding whether to give a patient fluid, nurses must understand the need for volume status and fluid responsiveness assessment. Assessing volume status necessitates determining whether the vascular volume is normal, increased, or decreased at a static point in time. Assessing fluid responsiveness requires examining a dynamic question: Will fluid administration increase stroke volume and cardiac output, which will then increase blood flow to the tissues? In addition, nurses must understand the concepts of vascular permeability and tone, cardiac contractility, and elasticity. Even stable patients might have a mild response to a fluid bolus and not be significantly hypovolemic.
Limitations
A nonrandom sampling presented a major limitation in this study. Voluntary participation creates a bias regarding the type of nurse who completes a survey. The fact that 929 nurses started the survey but only 291 completed it calls into question the type of respondent. The nurses who fully participated could be highly motivated and more knowledgeable, so the results may be even lower than reported.
Implications for nursing practice
The results of this study indicate that reliance on traditional, less-accurate measures of volume status and fluid responsiveness remain the norm. Our results indicate a call for action in analyzing nursing education content surrounding fluid management best practices. Offering a foundation of knowledge in undergraduate nursing curriculum provides a first step toward the application of nursing practice in individualized fluid management. The establishment of standards to determine the education or experience level necessary to care for a patient with fluid abnormalities will help ensure competency and skill. In addition, professional organizations could significantly enhance the provision of evidence-based education on fluid management by incorporating the data into materials used for nursing education.
Without a concerted effort by respected nursing organizations, the lack of understanding with regard to fluid volume and responsiveness can’t be resolved. The result of which will negatively impact patient outcomes.
Barbara “Bobbi” Leeper, a clinical nurse specialist in cardiovascular and critical care, works as an independent consultant in Dallas, Texas. Tom Ahrens is the chief learning officer at NovEx in St. Louis, Missouri. Chantal Toth is a clinical nurse specialist at Reading Hospital – Tower Health in West Reading, Pennsylvania. Kathleen Vollman is clinical nurse specialist/consultant at Advancing Nursing, LLC in Northville, Michigan.
Funding: Baxter International Inc. provided an unrestricted educational grant for this research.
American Nurse Journal. 2024; 19(5). Doi: 10.51256/ANJ052448
References
American Association of Critical-Care Nurses. Essentials of Critical Care Orientation. aacn.org/education/online-courses/essentials-of-critical-care-orientation?tab=Successful%20Completion
Burns D, Burns D, Shively M. Critical care nurses’ knowledge of pulmonary artery catheters. Am J Crit Care. 1996;5(1):49-54.
Connors AF Jr, Dawson NV, Shaw PK, Montenegro HD, Nara AR, Martin L. Hemodynamic status in critically ill patients with and without acute heart disease. Chest. 1990;
98(5):1200-6. doi:10.1378/chest.98.5.1200
Connors AF, Speroff T, Dawson NV, et al. The effectiveness of right heart catheterization in the initial care of critically ill patients. SUPPORT investigators. JAMA 1996;276(11):889-97. doi: 10.1001/jama.276.11.889
Crowe S. Understanding nursing perceptions of intravenous fluid management practices. Br J Nurs.2023;32(14):S36-40. doi:10.12968/bjon.2023.32.14.S36.
Douglas IS, Alapat PM, Corl KA, et al. Fluid response evaluation in sepsis hypotension and shock: A randomized clinical trial. Chest. 2020;158(4):1431-45. doi:10.1016/j.chest.2020.04.025
Hartjies T. AACN Core Curriculum for Progressive and Critical Care Nursing. 8th ed. Philadelphia, PA: Elsevier; 2022.
Iberti TJ, Daily EK, Leibowitz AB, Schecter CB, Fischer EP, Silverstein JH. Assessment of critical care nurses’ knowledge of the pulmonary artery catheter. The Pulmonary Artery Catheter Study Group. Crit Care Med. 1994;22(10):1674-8.
Iregui MG, Prentice D, Sherman G, Schallom L, Sona C, Kollef MH. Physicians’ estimates of cardiac index and intravascular volume based on clinical assessment versus transesophageal Doppler measurements obtained by critical care nurses. Am J Crit Care. 2003;12(4):336-42.
Kaufman DA, Lopes M, Maviya N, Magder SA. The ins and outs of IV fluids in hemodynamic resuscitation. Crit Care Med. 2023;51(10):1397-1406. doi:10.1097/CCM.0000000000006001
Kupchik N. Principles of resuscitation. Crit Care Nurs Clin North Am. 2021;33(3):225-44. doi:10.1016/j.cnc.2021.05.001
Parks JK, Elliott AC, Gentilello LM, Shafi S. Systemic hypotension is a late marker of shock after trauma: A validation study of Advanced Trauma Life Support principles in a large national sample. Am J Surg. 2006;192:727-31. doi:10.1016/j.amjsurg.2006.08.034
Key words: Fluid responsiveness, volume status, intervascular volume, stroke volume