Implementation strategies and considerations
- Virtual reality is a computer simulation system that creates an interactive, three-dimensional environment in which users experience a sense of physical presence via auditory, visual, and tactile stimuli.
- Research indicates that VR’s immersive nature can provide an effective means of distraction to aid increases in pain tolerance thresholds and decreases in perceived pain intensity, anxiety, and time spent thinking about pain.
Huang and colleagues define virtual reality (VR) as a computer simulation system that creates an interactive, three-dimensional environment in which users experience a sense of physical presence via auditory, visual, and tactile stimuli. A typical VR system consists of a head-mounted display that tracks the user’s head movements, handheld controllers that enable interaction with the virtual environment, and external speakers or headphones that deliver audio. Together they create a fully immersive virtual experience.
According to Chow and colleagues, VR can be active or passive depending on the level of interactivity. Active VR requires user engagement with handheld controls; passive VR allows users to assume an observer role as they watch a 360-degree movie or clip.
What’s the future of AI-assisted nursing?
Artificial intelligence in nursing
In the area of pain management, Eijlers and colleagues found greater pain reduction with active VR because of its immersive nature. Goudman and colleagues describe VR’s immersive nature as making it a more effective means of distraction compared to traditional measures, resulting in increases in pain tolerance thresholds, with concomitant decreases in perceived pain intensity, anxiety levels, and time spent thinking about pain. (See VR in healthcare.)
VR in healthcare
Ioannou and colleagues attribute virtual reality’s (VR’s) surge within healthcare to technological advancements that have enhanced affordability, flexibility, portability, and immersivity.
VR has been explored in pediatric and adult populations to treat acute and chronic pain, depression, fatigue, distress, and anxiety. A recent systematic review by Smith and colleagues found a statistically significant improvement in pain (67% of included studies) and anxiety (50% of included studies). VR’s efficacy in alleviating pain and anxiety has been demonstrated in numerous procedures and indications, including dentistry, burn care, surgery, oncology, venous and port access, trauma, labor pain, lumbar puncture, episiotomy repair, dressing changes, spinal cord injury, and chronic pain.
In addition to providing distraction, VR has a role in an array of therapeutic applications such as focus shifting, skill-building, mindfulness, meditation, relaxation, breath training, guided imagery, exercise, rehabilitation, exposure therapy, and patient education.
Smith and colleagues attribute VR’s effectiveness in treating pain to the following two theories: Gate Control Theory suggests that the perception of pain depends on the degree of attention allocated to the painful stimulus. The Multiple Resource Theory proposes that humans possess a finite capacity to process pain and suggests that diverting cognitive resources from the painful stimulus to the virtual environment can reduce pain perception
In anticipation of implementing VR in our organization, we conducted an extensive literature review and explored both internal and external evidence to better understand the technology and its use to manage pain and anxiety. The steps we took and barriers we surmounted might help you launch a similar program in your work setting.
Project development
Our multidisciplinary team of three RNs, one licensed acupuncturist from the integrative medicine department, and an advanced practice provider manager represented diverse settings, including adult, pediatric, acute care, ambulatory care, pain management, medical-surgical, and integrative medicine. The team mentors (clinical nurse specialist and a pain management physician) provided guidance and expertise.
Problem identification and clinical inquiry
As opioid overdose rates continue to rise in the United States, the Centers for Disease Control and Prevention (CDC) recommends that clinicians maximize nonpharmacologic therapies. Due to its low incidence of dizziness, headache, nausea, and eye strain, VR offers an innovative, low-risk intervention to treat pain and other related symptoms.
Ioannou and colleagues suggest that VR can supplement or replace traditional pharmacologic therapies to adequately treat pain in various settings. By reducing exposure to or consumption of pain medications, VR has the potential to decrease medication-related side effects, length of stay, and healthcare costs.
Evidence review
We developed the following PICO(T) (Population, Intervention, Comparison or Control, Outcome, Time) question to guide our literature search: “In adult and pediatric patients, how does the application of VR, as compared to its absence, influence pain or anxiety?” Our literature review resulted in 30 relevant articles.
The subsequent evidence synthesis process involved systematically evaluating primary and secondary outcomes, potential side effects, clinical settings, patient populations, regional variations, device manufacturers, and the practical applications of VR. The primary outcomes we explored included pain intensity, anxiety severity, cognitive preoccupation with pain, and pain medication requirements. Secondary outcomes encompassed range of motion, patient and provider satisfaction, quality of life, procedural duration, and distress levels.
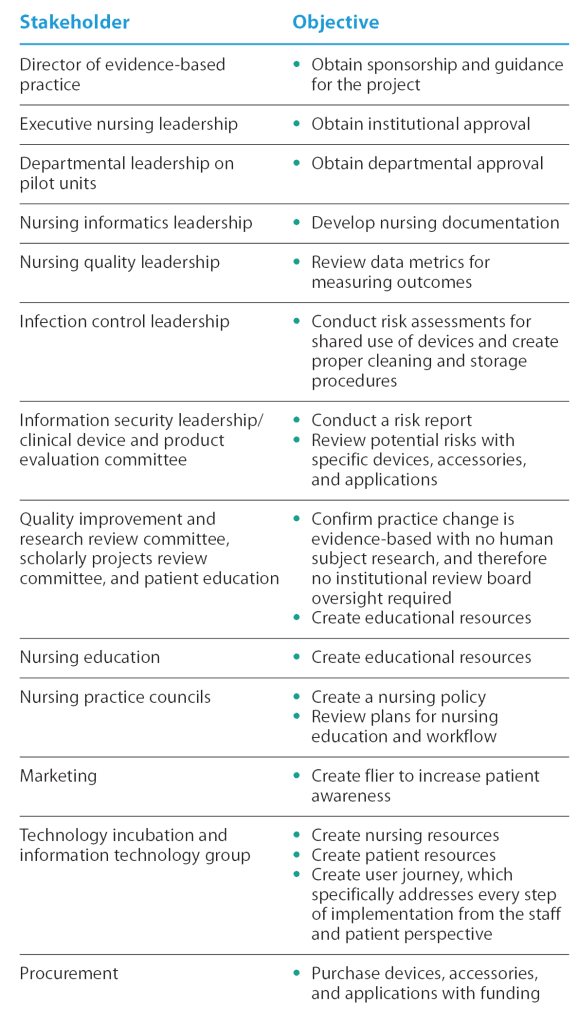
Stakeholder buy-in
Successful implementation of any nursing project or practice requires collaboration with and buy-in from relevant stakeholders, as well clear objectives. At our organization, those stakeholders included the following:
In parallel, we gathered internal and external evidence to comprehend current VR-related practices within and outside our organization. We collaborated with our organization’s information technology team, which had prior VR experience, and two external nurse-led teams that had successfully incorporated VR into their standard practices. These conversations helped us better understand and anticipate specific barriers to implementation, including those related to patients (selection, inclusion/exclusion criteria, education), providers (patient identification, staff education, staff buy-in), and devices (storage, troubleshooting, cost, infection control).
Evidence-based practice recommendations
Based on the synthesized evidence, we recommend using VR as a complementary or adjuvant intervention to treat pain or anxiety in pediatric and adult populations. Following an extensive evaluation of various products and manufacturers, we selected Oculus Quest 2 because of its affordability, user-friendly interface, and portability. In adherence with the manufacturer’s recommendations, we advised VR use for patients age 13 years and above. Per the evidence-based practice model, we encouraged patient preference by procuring a diverse array of VR applications for patient autonomy. We also considered patient safety, so we ensured availability of varying levels of interactivity. This was particularly necessary in the case of procedures that may limit patient movement, which will necessitate adaptations to VR use.
Project implementation
Implementation of this project required several steps, including stakeholder buy-in, to ensure success. (See Stakeholder buy-in.)
Unit and population selection
We initiated implementation of the project by selecting the pilot unit and population of interest. Given the evidence supporting the use of VR for both adult and pediatric populations, we chose the adult ambulatory pain service and pediatric day hospital. These units regularly perform procedures that provoke pain and anxiety among patients. An RN on our team who worked within these units facilitated efficient oversight of the VR implementation process.
Cost-savings analysis
We revised the costs associated with the initiative, including for the devices, accessories, and applications. Savings related to the project include potential reduction in medication requirements, which would help decrease medication-related side effects and length of stay.
Nursing policy
Because our organization hadn’t yet implemented VR, we created a nursing policy. The policy provides nursing staff with information regarding the appropriate population and indications; background and supporting evidence; exclusion criteria; nursing assessment; patient education; required equipment; procedural steps for cleaning, set-up, and use; storage; device maintenance; and documentation. (See Exclusion criteria.)
Exclusion criteria
Based on manufacturer recommendations and supporting scientific evidence, we developed the following exclusion criteria for virtual
reality use.
- Individuals with a history of motion sickness, vertigo, seizures, migraines, or skin hypersensitivity
- Children under 13 years
- Patients experiencing acute issues, including nausea/vomiting, headache, respiratory symptoms, ocular infections, or ocular irritation
- Patients with acute delirium
- Patients with cardiac pacemakers or hearing aids
- Patients with open facial or cranial wounds
- Individuals who exhibit an inability to communicate effectively
- Patients diagnosed with severe mental illness
- Patients with visual or auditory impairment
- Individuals currently under active infection control precautions
- Patients undergoing their initial chemotherapy infusion
- During procedures that require the patient to be in a prone position
- During imaging procedures such as magnetic resonance imaging, magnetic resonance linear accelerator, or positron emission tomography
Patient and nurse education
We created a written patient education resource in English, Spanish, and Russian. It includes a definition of VR, indications and directions for its use, and contraindications.
Before initiating nurse education, we conducted several dry runs to preemptively address any potential issues or barriers that might surface during the actual implementation. We also identified superusers within each pilot unit to facilitate the staff education process and streamline subsequent VR implementation.
Staff education consisted of written materials, a learning module, and simulation. The written resources included step-by-step guides with images and descriptions for set-up, use, cleaning, documentation, and storage. During the simulation phase, we paired nurses and assigned them roles as caregiver and patient to foster a comprehensive understanding of both perspectives.
After the learning module and simulation, we used a competency checklist to ensure nurse understanding of all implementation elements, including nursing policy, patient selection, patient education, site assessment, required equipment, device use, set-up/cleaning procedure, and documentation.
To aid in the selection of suitable VR applications for use with individual patients, we distributed a guide with an overview of each available application, including the appropriate patient population, specific features, and level of interactivity.
Measurable outcomes
We measured both staff and patient outcomes. To compile and manage staff outcomes, we used Research Electronic Data Capture, which is hosted within our organization. Pre- and post-educational surveys evaluated staff knowledge, competency, and willingness to use VR technology. We also developed post-implementation surveys to assess the length of VR use appointments, staff satisfaction, ease of use, willingness to use, and barriers/facilitators to implementation.
To determine patient-reported outcomes, we worked with the organization’s nursing quality, nursing informatics, and nursing practice stakeholders. The patient-reported outcomes included pain intensity, adverse events, time using VR, patient satisfaction, and willingness to use VR again.
Budget and funding
Our budget consisted of equipment needed for implementation, including the devices, additional accessories to ensure adherence with infection control recommendations, and applications. We applied for internal and external grant funding.
We purchased the Oculus Quest 2 (now called the Meta Quest 2) and accessories. Per infection control recommendations related to shared use, we also purchased hard, wipeable interface brackets and head straps; disposable face masks; and disposable hair bouffant caps. We selected applications based on numerous factors, including indication (distraction, breath training, relaxation), population (pediatric and adult content), and level of interactivity (passive to immersive).
Collaboration
Our technology incubation team (product manager, product designer, and software engineer) served as our most involved stakeholder. They proved instrumental in implementation, assisted with understanding device functionality, identified potential applications, and constructed patient and staff resources. Together, we created a user journey that describes every step of the implementation process before, during, and after VR use.
Challenges
While developing and implementing this practice change from 2019 to 2023, we encountered several unforeseen obstacles, mainly precipitated by the COVID-19 pandemic. Infection control (particularly with regard to shared device use) proved the primary impediment to successful VR implementation. Because the selected VR device is designed for individual or home use, we collaborated closely with our infection control department to establish an appropriate cleaning protocol and ensure safe use among multiple patients. We replaced the standard foam interface bracket and soft head strap with hard, easily cleanable alternatives. We also mandated wearing disposable face masks and hair bouffant caps.
We also encountered challenges with financial support. To offset budgetary constraints, we secured grant funding from an internal nursing fund dedicated to supporting nursing-led initiatives aimed at enhancing patient care. Our limited budget influenced our choice of VR device and the extent of our implementation plan, which lead us to forego any subscription models. Initially, we had envisioned an organization-wide implementation; however, due to restrictions on the number of devices procured, we limited implementation to two units.
Collaborate and anticipate
VR offers a cost-effective, low-risk intervention to treat pain or anxiety in pediatric and adult populations. Using visual, tactile, and auditory stimuli aids distraction, focus shifting, skill-building, mindfulness, meditation, relaxation, breath training, guided imagery, exercise, rehabilitation, exposure therapy, and patient education. Working closely with major stakeholders within your organization and addressing anticipated barriers can support successful implementation of this evidence-based pain and anxiety management intervention.
The authors work at Memorial Sloan Kettering Cancer Center in New York City, New York. Kelly Preti is a nurse practitioner, Maria Pinero is a clinical nurse IV, Matthew Weitzman is the lead acupuncturist, and Vivek Malhotra is chief of the pain service.
Financial disclosure: This work was supported in part by a Memorial Sloan Kettering Cancer Center Support Grant/Core Grant (Grant No. P30 CA008748) through funding from the National Cancer Institute and by Memorial Sloan Kettering Cancer Center Geri & ME Nursing Fund.
American Nurse Journal. 2024; 19(5). Doi: 10.51256/ANJ052442
References
Ahmadpour N, Randall H, Choksi H, Gao A, Vaughan C, Poronnik P. Virtual reality interventions for acute and chronic pain management. Int J Biochem Cell Biol. 2019;114: 105568. doi:10.1016/j.biocel.2019.105568
Chow H, Hon J, Chua W, Chuan A. Effect of virtual reality therapy in reducing pain and anxiety for cancer-related medical procedures: A systematic narrative review. J Pain Symptom Manage. 2021;61(2):384-94. doi:10.1016/j.jpainsymman.2020.08.016
Czech O, Wrzeciono A, Rutkowska A, Guzik A, Kiper P, Rutkowski S. Virtual reality interventions for needle-related procedural pain, fear and anxiety—A systematic review and meta-analysis. J Clin Med. 2021;10(15):3248. doi:10.3390/jcm10153248
Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC Clinical Practice Guideline for Prescribing Opioids for Pain—United States, 2022. MMWR Recomm Rep. 2022;71(3):1-95. doi:10.15585/mmwr.rr7103a1
Eijlers R, Utens EMWJ, Staals LM, et al. Systematic review and meta-analysis of virtual reality in pediatrics: Effects on pain and anxiety. Anesth Analg. 2019;129(5):1344-53. doi:10.1213/ANE.0000000000004165
Goudman L, Jansen J, Billot M, et al. Virtual reality applications in chronic pain management: Systematic review and meta-analysis. JMIR Serious Games. 2022;10(2):e34402. doi:10.2196/34402
Huang Q, Lin J, Han R, Peng C, Huang A. Using virtual reality exposure therapy in pain management: A systematic review and meta-analysis of randomized controlled
trials. Value Health. 2022;25(2):288-301. doi:10.1016/j.jval.2021.04.1285
Ioannou A, Papastavrou E, Avraamides MN, Charalambous A. Virtual reality and symptoms management of anxiety, depression, fatigue, and pain: A systematic review. SAGE Open Nurs. 2020;6:2377960820936163. doi:10.1177/2377960820936163
Mallari B, Spaeth EK, Goh H, Boyd BS. Virtual reality as an analgesic for acute and chronic pain in adults: A Systematic review and meta-analysis. J Pain Res. 2019;12:2053-85. doi:10.2147/JPR.S200498
Meta. Welcome to the Meta Quest safety center. 2023. oculus.com/safetycenter/#:~:text=Designed%20for%20Age%2013%2B,or%20use%20Meta%20VR%20Systems
Smith V, Warty RR, Sursas JA, et al. The effectiveness of virtual reality in managing acute pain and anxiety for medical inpatients: Systematic review. J Med Internet Res. 2020;22(11):e17980. doi:10.2196/17980
Key words: virtual reality, pain, anxiety